
Those precious few minutes between patients can feel like a race against time. If you’re anything like me, you’re already running a few minutes behind; there are a thousand chart notes swirling in your head; you have to get the room properly disinfected, devices sterilized, and the room reset before you seat the next patient (and you also have to pee!). You go into autopilot. Kind of like on the drive home when you’re suddenly in your driveway and don’t remember how you got there. Were you safe along the way? Could you have run a stop sign?
The same could be true for your operatory turnover. Were you wearing the proper PPE? Did you clean and disinfect all the clinical contact surfaces? Did they stay wet for the appropriate kill time? Is your operatory safe for you and your next patient?
The Organization for Safety, Asepsis and Prevention (OSAP) just released a new version of “If Saliva Were Red.” Think back to the first time you saw that iconic video and realized the importance of proper room turnover. I think back to my first time in hygiene school; it took me over an hour to disinfect the operatory. There’s a lot to think about between direct contact, spatter, droplets, and aerosols. In our rush to get that next patient in the chair, have we taken the time to understand how our disinfectant is supposed to be used?
You might also be interested in:
Dental aerosols and the pandemic: A necessary wake-up call
Dental unit waterlines: Trickier than you think
I will say that I have not put much thought into the disinfectant that’s in my operatory; I’ve treated them all pretty much the same and probably didn’t notice if the products changed. But it’s time to take a precious second and understand the nuances of the surface disinfectants in your op for the safety of you and your patients, and for care of your equipment.
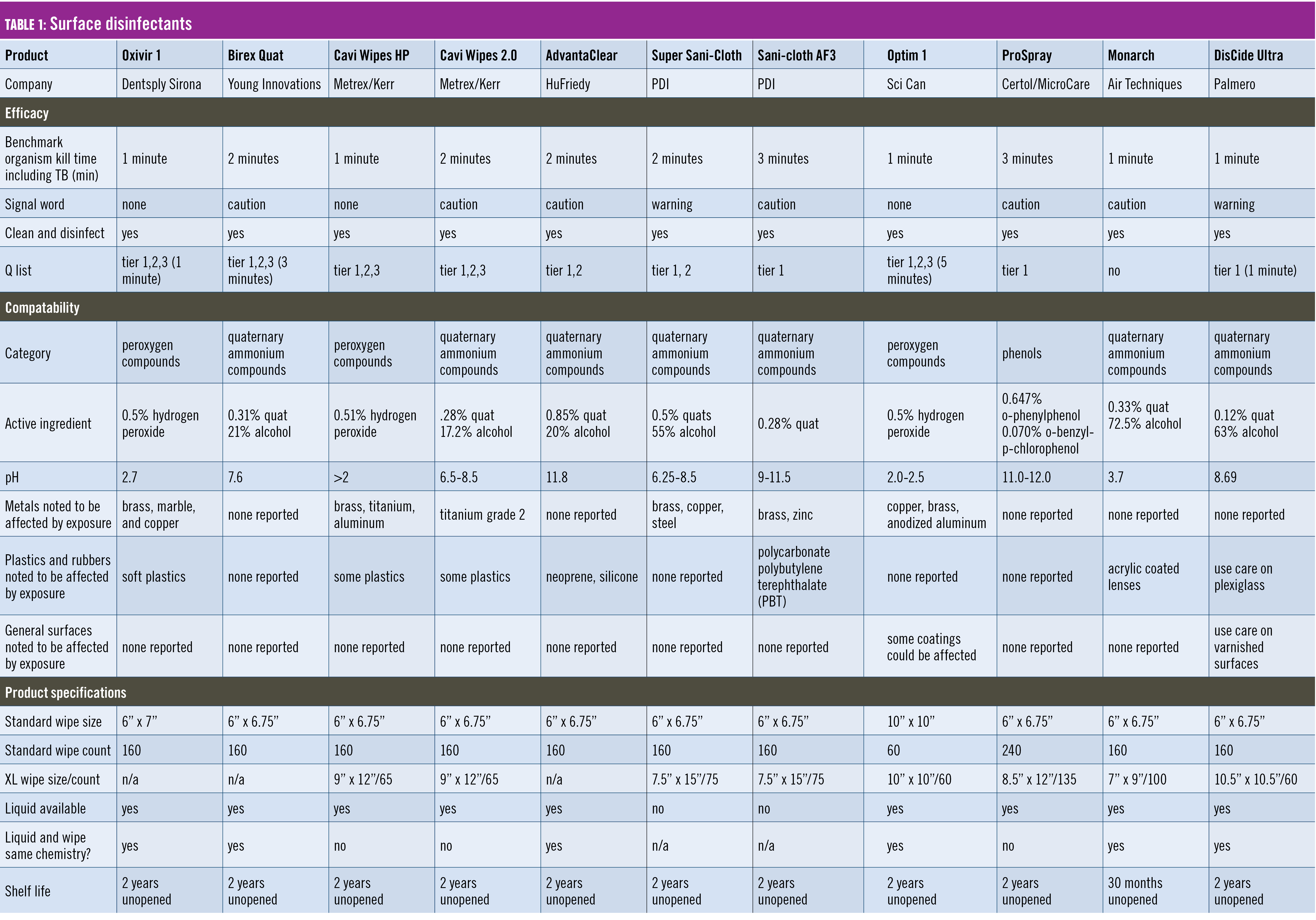
So, what exactly do we need in a disinfectant? We need it to kill organisms in a reasonable amount of time, be safe for the user, and be the least harmful to our equipment. That’s a tall order.
Spoiler: there is no perfect product. Disinfectants are created to be destructive to cells, so none are completely harmless. The EPA denotes a product’s toxicity with signal words if deemed necessary. Some popular wipes say WARNING, meaning moderately toxic, or CAUTION, indicating low toxicity.
Kill contaminants
The CDC requires an intermediate-level, hospital-grade surface disinfectant with a TB claim for any surface that is contaminated with blood.1 Since TB is the hardest to kill, that’s the benchmark used in selecting a disinfectant. There are disinfectant wipes intended for health care without a TB claim, so be sure to look at the label.
We all learned spray-wipe-spray or wipe-discard-wipe (note the same wipe cannot clean and disinfect. You must use more than one). Cleaning removes any bioburden so that the disinfectant can do its job. If there is any matter in the way, the product will not disinfect.

Ensure your wipe can both clean and disinfect. Any wipe that claims one step only refers to the disinfectant part. The surface must be clean before disinfection, so you can call that one step (meaning disinfect after you’ve cleaned) or two step (clean and disinfect); that part is semantics. But you can’t skip the clean part. You might be tempted to choose the disinfectant that kills the most bugs, like ones you would find only in a vet’s office. It’s great marketing, but in practice, as long as it kills the stuff you need it to, it’s good.
Product labeling can be confusing. It might say “one-minute kill time” in bold on the front with a little cross or asterisk next to it leading to the fine print on the back that says “only for HIV and HBV,” and the TB kill time is two minutes. The surfaces you’re disinfecting must stay wet for the entire TB kill time to disinfect properly. That might mean going back with another wipe or two or three. But don’t fall into the trap that more product is better. There’s a sweet spot; more is not only wasteful but also makes a mess and could harm expensive equipment.
Another thing to consider when choosing a product is emerging pathogens. Remember when we all scrambled to see if our wipe killed COVID-19? In reaction, the EPA created List N to show which products killed COVID-19, and it now has List Q. You can enter the EPA number found on your product and see if it is approved to kill emerging tier 1, 2, and/or 3 viruses. That way, if another pathogen threatens us, we know if our product can do the job.
Surface compatibility
This one is tough. While the EPA closely regulates what organisms a disinfectant kills, the effect on surfaces works on the honor system—meaning each disinfectant manufacturer decides how they want to evaluate and share how their product interacts with your equipment.
Understanding how each active ingredient affects surfaces can help you make your choice. The higher percentage of an active ingredient, the faster the kill time, and the further from a neutral pH usually means more potential for surface interaction. Each category of disinfectant has some pros and cons.
Understanding the different types of disinfectants
Today’s most common disinfectant categories used in dentistry are quaternary ammonium compounds (quats), alcohols, phenols, and peroxygen compounds. Just because they’re in a group together does not mean they are the same. Each product contains varying concentrations of active and inactive ingredients affecting how it works and interacts with the environment around you.
Quaternary ammonium compounds: Also known as quats, this active ingredient is often combined with alcohol to improve kill time for a broader spectrum of microorganisms. Alcohol by itself, while capable of disinfection, dries quickly and can damage plastics. Quat-alcohol combos have a relatively quick TB kill time, but their surface compatibility varies greatly by the concentration of ingredients. Higher alcohol contents can have more interactions. Quats have been reported to cause respiratory and skin irritation in high concentrations.
Phenols: Phenols are one of the oldest disinfectant compounds, starting with carbolic acid and Joseph Lister in the 1880s. They have evolved since then and remain an effective but lesser-used disinfectant. They tend to have a longer kill time and leave behind a residue that requires periodic washing. However, that’s not all bad because every disinfectant leaves behind some kind of residue, and routine washing can go a long way toward equipment longevity.
Peroxygen compounds: Hydrogen peroxide compounds are considered more environmentally friendly and have fast-acting kill times. Some even claim you don’t need to wear PPE when handling them, but please don’t start doing bare-handed room turnover. You’re still dealing with bloodborne pathogens and sharp instruments, so keep yourself safe and don the PPE. These compounds typically have a pH of 3 or lower, and have been reported to interact with metals, plastics, and upholstery.
Never skip the PPE
Speaking of PPE, OSHA and the CDC both say that clinicians should wear puncture-resistant “heavy-duty” gloves, mask, and protective eyewear for cleaning, sterilizing, and disinfecting treatment rooms and equipment.1,2 Remember what these disinfectants do—destroy cells. So you need to protect yourself from these hazards.
Check your instructions for use (IFU)
Ask an equipment manufacturer what product to use, and you’ll get a different answer depending on who you ask. If you take the time to read the IFU for, say, your operatory chair, you might find it recommends a category of disinfectant to use or even which product. (You also might find, conveniently, that company also makes that disinfectant.)
If you read all the IFUs of all your different equipment, you could end up with several disinfectant recommendations. You don’t want to void a warranty by using the wrong product. When in doubt, contact your equipment manufacturer for details on what compatibility testing they completed.
Don’t mix formulations
Now you’re thinking you need at least one of each category of disinfectants on your counter, right? Hold on. Mixing disinfectants, even those in the same class, even the same brand, can be dangerous to your health and destructive to your equipment. Think of the volcano back in middle school. Mix baking soda and vinegar, and you get an explosion.
While things certainly won’t explode, you could cause damage and potentially ruin your equipment or inhale something harmful. If you are a fan of mixing sprays and wipes, be sure they are the exact same formulation. Next time your sales rep walks in and tells you about this great sale on wipes, clean all your equipment with soap and water to remove any residue before switching, or say no thanks!
All of a sudden, that canister of wipes on your counter is a whole lot more complex. Understanding how to choose and use the wipe on your counter will go a long way toward protecting your patients, your equipment, and you.
And, for goodness’ sake, close the cap. A dry wipe won’t kill anything!
Editor's note: This article appeared in the May 2023 print edition of RDH magazine. Dental hygienists in North America are eligible for a complimentary print subscription. Sign up here.
References
- Guidelines for infection control in dental health-care settings—2003. Centers for Disease Control and Prevention (CDC). Accessed February 24, 2023. https://www.cdc.gov/mmwr/PDF/rr/rr5217.pdf
- FAQ - Personal Protective Equipment (PPE) – 2015. The Organization for Safety, Asepsis and Prevention (OSAP). Accessed February 24, 2023. https://www.osap.org/page/FAQPPE20154/index.php






{kind=link}